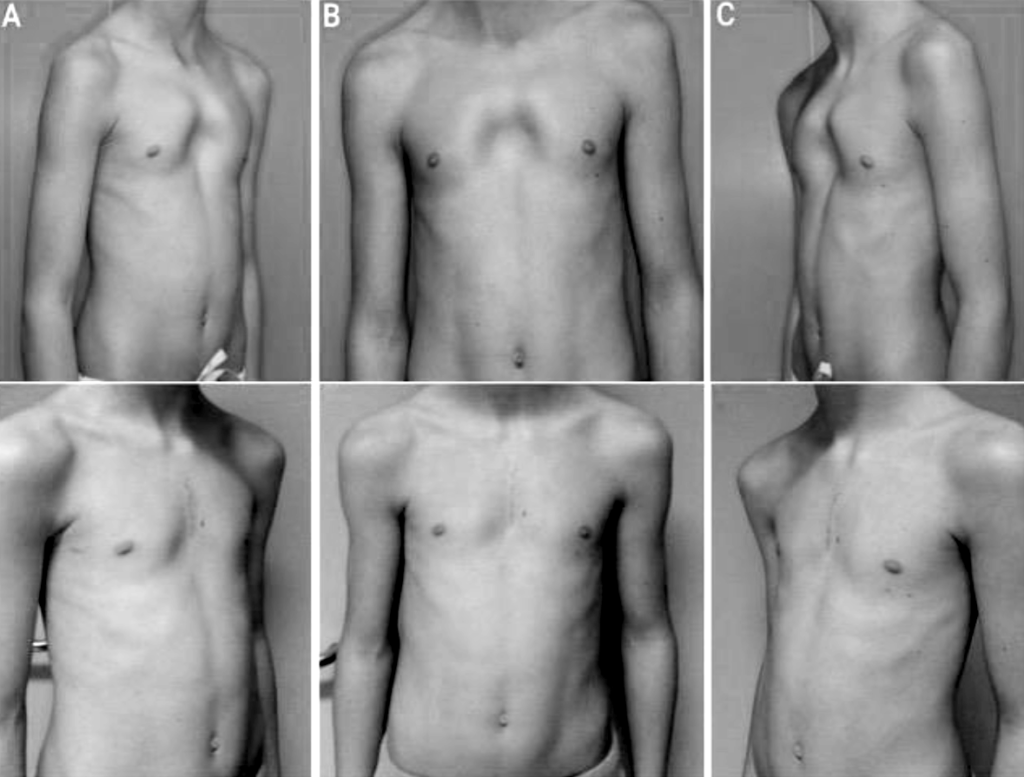
The pectus arcuatum (PA), also known as Currarino-Silverman syndrome, or type II deficient chest, is a rare congenital deformity of the chest wall characterized by the protrusion and early ossification of the sternum.
Current surgical correction strategies are minimally invasive and aim to reposition the sternum in its “correct” position.
The wedge sternotomy is performed at the most protruding point of the sternum, trying to preserve the posterior base of the sternum (in direct contact with the heart) and the periosteum
It may be difficult to obtain a satisfactory result in current clinical practice, as determining the correct intraoperative cutting angle often involves the need to adjust the oscillating cutting saw, with the risk of intraoperative complications and over- or under-correction of the deformity. When this happens, bone or cartilage grafts are used to fill in the gaps left after sternotomy [4].
In this context, the availability of a customized surgical template capable of constraining the optimal cutting angle allows the aesthetic outcome to be drastically improved and, at the same time, surgical time and intraoperative complications to be reduced and the use of bone or cartilage grafts to be avoided.
Technology
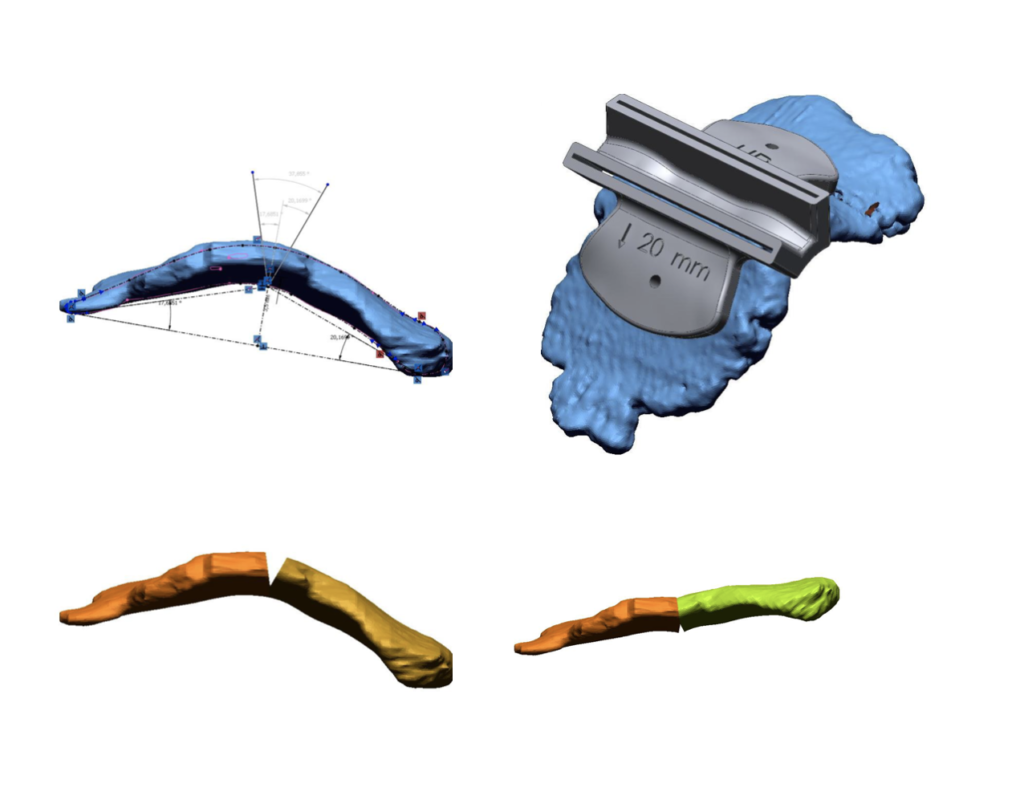
To create a tailor-made cutting template for the individual patient’s wedge-shaped sternotomy, we started with a CT scan which was then processed to create a 3D virtual reconstruction of the patient’s sternum. At the most prominent point of the defect, the angle that allows both optimal realignment of the sternum and preservation of the posterior bone cortex of the sternum is obtained geometrically through an automated process. The 3D model is then used to create a virtual surgical template, adapted to the upper face of the sternum. Its design consists of: two holes to insert the titanium screws, to fix the template to the sternum, and two slots to guide the insertion of the oscillating force saw according to the calculated angle. The slots contain a safety lock to prevent the blade from exceeding the rear periosteum, to preserve it. The blade is stopped 3 to 5 mm above the posterior bone plate, depending on the thickness. After virtually simulating the resection, in order to verify the adaptability of the mask to the patient’s sternum and confirm that the sternal realignment is correct, both the sternum and the mask are printed, allowing surgeons to simulate the procedure before the actual procedure. The cutting template is then printed in titanium alloy and sterilized for intraoperative use.
Clinical experience
The cutting template thus created has been used in four operations for the surgical treatment of PA. No intraoperative complications were found and post-operative chest X-rays of all four patients showed optimal sternal realignment and stabilization. At follow-up, post-operative images showed an optimal esthetic result with a high degree of patient satisfaction.